For decades, the success of organ transplantation has been tempered by a Faustian bargain: a life-saving organ in exchange for a lifetime of immunosuppressant drugs. These regimens, while effective at preventing the body from rejecting a foreign organ, leave patients vulnerable to opportunistic infections and chronic conditions including diabetes, kidney failure, and certain cancers. The central ambition of transplant medicine — immune tolerance, in which a recipient's body learns to recognize a donor organ as its own — has remained elusive since the first successful kidney transplant in the 1950s.
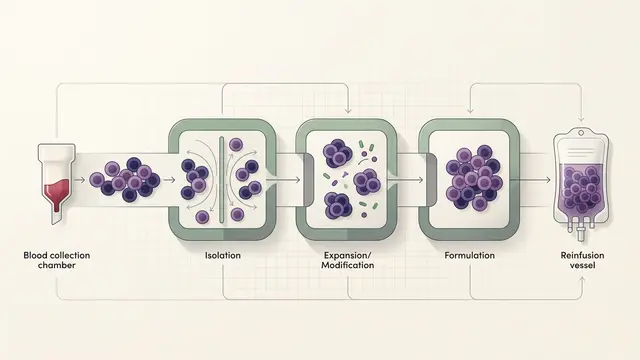
A small, early-stage study published in Nature Communications now offers a concrete step toward that goal. Researchers focused on living-donor liver transplants, a procedure that takes advantage of the liver's unique capacity to regenerate. By harvesting white blood cells from the donor and engineering them in a laboratory into "regulatory dendritic cells," the team created a bespoke cell therapy designed to train the recipient's immune system to accept the transplanted tissue rather than attack it.
From blunt suppression to biological precision
The conventional approach to preventing organ rejection relies on calcineurin inhibitors, corticosteroids, and other systemic immunosuppressants that broadly dampen the immune response. The trade-off is well documented: patients gain organ function but lose a significant degree of immune competence, often for the rest of their lives. Long-term immunosuppression is associated with elevated rates of infection, cardiovascular disease, metabolic disorders, and malignancies — side effects that accumulate over years and that transplant physicians have long regarded as an unavoidable cost of the procedure.
The dendritic cell approach described in the study represents a fundamentally different logic. Dendritic cells serve as sentinels of the immune system, presenting fragments of foreign material to T cells and effectively deciding whether to trigger an immune attack or promote tolerance. By engineering donor-derived dendritic cells into a regulatory phenotype — one that signals tolerance rather than alarm — the researchers aim to intercept the rejection cascade before it begins. This contrasts with earlier experimental work centered on regulatory T cells, which sought to suppress immune responses after activation rather than prevent them at the point of antigen presentation.
The distinction matters. Regulatory T cell therapies have shown promise in early trials but face challenges of scalability, persistence, and specificity. Dendritic cells occupy an upstream position in the immune signaling chain, which in principle allows them to shape the response more broadly and more durably. Whether that theoretical advantage translates into clinical superiority remains an open question, but the mechanistic rationale is coherent.
The liver as proving ground
The choice of liver transplantation as the setting for this research is not incidental. The liver is considered an immunologically privileged organ — it naturally harbors mechanisms that promote tolerance, a property thought to have evolved because the organ is constantly exposed to foreign antigens from the gut via the portal vein. Liver transplant recipients already tend to require lower doses of immunosuppression than recipients of kidneys or hearts, and a small but documented subset of liver recipients have been successfully weaned off immunosuppressants entirely over time.
This immunological backdrop makes the liver an attractive testing ground for tolerance-inducing therapies. If regulatory dendritic cells can push the balance further toward acceptance in liver recipients, the question becomes whether the same approach can extend to organs with less forgiving immunological profiles — kidneys, hearts, lungs — where rejection pressures are more aggressive and the clinical need for alternatives to lifelong drug regimens is arguably even greater.
The study is preliminary, and the gap between early-phase results and standard clinical practice in transplant medicine is wide. Cell therapies of this kind face significant hurdles in manufacturing consistency, regulatory approval, and cost. Yet the underlying shift it represents — from pharmacological suppression of the entire immune system to the targeted re-education of its decision-making architecture — aligns with a broader movement in medicine toward biological specificity. The tension now sits between the elegance of the concept and the practical complexity of delivering personalized cell therapies at the scale transplant medicine demands.
With reporting from STAT News.
Source · STAT News (Biotech)