Actor Sam Neill recently announced that he is cancer-free after participating in a clinical trial for CAR T-cell therapy, a milestone that highlights the efficacy of advanced immunotherapy. After conventional chemotherapy failed to address his stage-three blood cancer, Neill turned to this experimental treatment, which has now yielded a positive clinical outcome. According to reporting from The Guardian, Neill is currently leveraging his public platform to advocate for the broader availability of this therapy within Australia’s healthcare infrastructure.
The case serves as a high-profile illustration of the transition from generalized chemical interventions to highly specific, personalized cellular therapies. While the medical community has long understood the potential of immunotherapy, the successful application of CAR T-cell technology in complex hematological cases suggests that we are entering a new phase of oncology where the patient’s own immune system is engineered to recognize and neutralize malignancy. This development necessitates a critical evaluation of how medical systems transition from experimental trials to standardized, accessible care.
The Evolution of Precision Immunotherapy
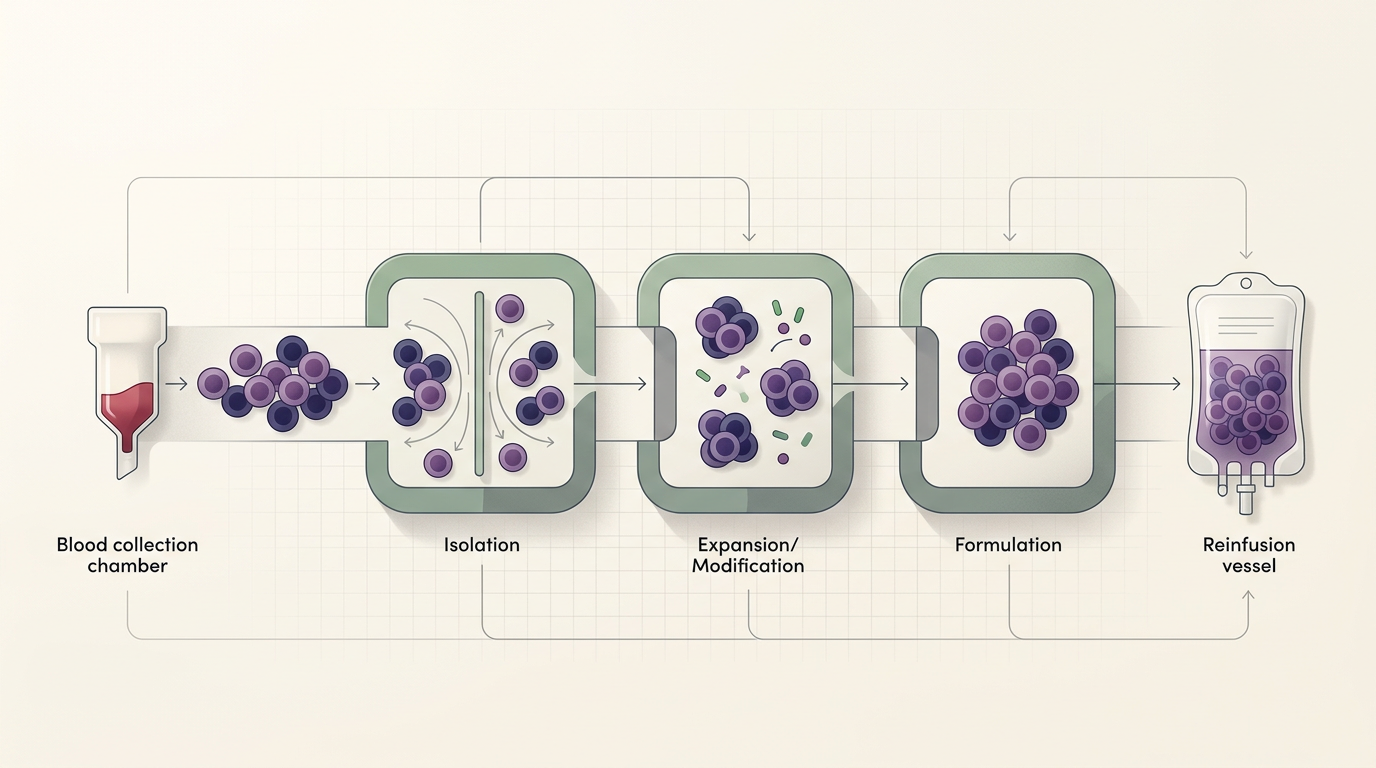
CAR T-cell therapy, or Chimeric Antigen Receptor T-cell therapy, represents a fundamental departure from traditional systemic treatments like chemotherapy or radiation. Unlike these conventional methods, which often function by indiscriminately targeting rapidly dividing cells—thereby causing significant collateral damage to healthy tissue—CAR T-cell therapy is a form of adoptive cell transfer. Clinicians extract a patient’s own T-cells, genetically modify them in a laboratory setting to express receptors that target specific proteins found on the surface of cancer cells, and then reinfuse these enhanced cells back into the patient.
The structural complexity of this process is what makes it both revolutionary and inherently difficult to scale. Because each treatment is bespoke, the logistical burden of manufacturing, quality control, and administration is vastly higher than that of mass-produced pharmacological agents. Historically, such therapies were confined to the most refractory cases where all other options had been exhausted. However, the success observed in patients like Neill is shifting the conversation toward earlier intervention, challenging the current clinical paradigm that reserves advanced immunotherapy for end-stage scenarios.
This shift is not merely clinical but also economic. The integration of personalized medicine requires a rethink of how hospital systems allocate resources. Unlike a bottle of medication that can be stocked on a shelf, a CAR T-cell regimen requires a sophisticated network of apheresis centers, specialized laboratories, and clinical expertise. The transition from a niche experimental procedure to a standard of care demands significant investment in infrastructure that many public health systems are currently ill-equipped to provide on a mass scale.
The Mechanics of Patient-Specific Outcomes
The efficacy of CAR T-cell therapy hinges on the precision of the genetic engineering involved. By programming T-cells to identify specific tumor antigens, clinicians effectively turn the body’s internal defense mechanism into a precision-guided weapon. This mechanism is particularly effective in blood cancers, such as leukemia and lymphoma, where the target antigens are often well-defined and accessible within the circulatory system. The success in these domains has provided a proof-of-concept that researchers are now attempting to translate to solid tumors, though the latter presents a significantly more complex microenvironment.
Beyond the biological mechanism, there is the incentive structure of clinical trials. The participation of high-profile individuals in such trials often accelerates the visibility and, by extension, the funding and regulatory attention directed toward these therapies. When a patient reports a successful outcome after traditional methods have failed, it creates a powerful narrative that can influence public policy and health expenditure. However, this also introduces a tension between the excitement surrounding 'miracle' outcomes and the reality of rigorous, evidence-based scaling. The challenge lies in ensuring that the enthusiasm generated by anecdotal success does not outpace the longitudinal data required to understand long-term side effects and durability of response.
Furthermore, the manufacturing process itself is a bottleneck. Because the therapy is derived from the patient, it is essentially a 'batch of one.' This necessitates a highly efficient supply chain that can move biological samples from a patient to a laboratory and back again without degradation. Any delay in this process can be fatal for a patient with rapidly progressing disease, highlighting why the logistical component of the treatment is just as critical as the biological one.
Implications for Stakeholders and Regulators
For regulators, the primary challenge is balancing the need for rigorous safety standards with the imperative to provide patients with life-saving access to innovative treatments. As clinical success stories multiply, the pressure to expedite regulatory approval for CAR T-cell therapies will intensify. Regulators must determine how to maintain clinical oversight while allowing for the rapid iteration of these personalized protocols. This involves a delicate navigation of risk-benefit ratios, particularly when dealing with patients who have exhausted all standard-of-care options.
Competitors in the pharmaceutical and biotechnology space are also facing a strategic shift. The rise of cell-based therapies is disrupting the traditional blockbuster drug model, where a single molecule is marketed to millions of patients. Instead, the future of oncology appears to favor companies that can master the 'platform'—the manufacturing and engineering infrastructure required to deliver personalized treatments at scale. This favors firms that can integrate the entire value chain, from the initial diagnostic biopsy to the final reinfusion of engineered cells, creating a new form of competitive moat based on logistical excellence rather than just intellectual property.
Future Outlook and Uncertainties
The long-term durability of CAR T-cell therapy remains an open question that will define its role in future oncology. While initial remission rates are promising, the medical community is still gathering data on how long these engineered T-cells persist and whether they can prevent recurrence over several years. Furthermore, the issue of accessibility remains a significant hurdle. If these treatments are only available to a subset of patients in high-income regions, it will exacerbate existing disparities in health outcomes, creating a two-tiered system of cancer care.
As we look forward, the focus will likely shift toward 'off-the-shelf' CAR T-cell therapies, which use donor cells instead of the patient’s own, potentially reducing both the cost and the time required for treatment. Whether these allogeneic therapies can achieve the same level of efficacy and safety as their autologous counterparts is the next great hurdle for the sector. The success of individual patients provides the momentum, but the sustained transformation of cancer treatment will depend on solving the systemic, logistical, and economic complexities that remain deeply embedded in the current medical landscape.
As the medical community continues to refine these personalized interventions, the broader question remains how to integrate such high-cost, high-complexity therapies into sustainable public health models. The trajectory of CAR T-cell therapy suggests that the future of medicine will be increasingly granular, but the path to universalizing that precision remains a work in progress that requires both scientific innovation and institutional adaptation.
With reporting from The Guardian
Source · The Guardian Science